More Vigilant Cardiac Care Today Leads to Fewer Costs Tomorrow
Cardiovascular diseases (CVD) affect nearly half of all American adults, and in addition to their impact on health outcomes, they have significant economic implications. 17% of all annual healthcare costs in the U.S. are associated with these conditions, the largest across all disease categories. In 2018, cardiovascular outcomes researcher Dr. Leslee Shaw and her collaborators published “10-Year Resource Utilization and Costs for Cardiovascular Care.” Four years on, it is still among the most extensive studies measuring the progression of cardiovascular diseases among initially healthy individuals and associating the costs of treating CVD with different risk factors.
Connecting Risk Factors to Costs
The Shaw study reviewed 6,814 asymptomatic participants from the Multi-Ethnic Study of Atherosclerosis (MESA) sponsored by a NIH National Heart, Lung, and Blood Institute. Her study examined expenditures connected to:
- CVD medications
- Office visits
- Diagnostic procedures
- Coronary revascularizations
- Hospitalizations
The study’s cost figures were derived from Medicare nationwide and zip-code-specific data that was inflation-corrected, discounted at 3% per year, and presented in 2014 dollars.
Methodology
Each participant completed a baseline visit at the beginning of the study where they self-reported their “history of diabetes, hyperlipidemia, hypertension, family history of CVD and smoking history.” They also had their lipids, glucose, blood pressure, high-sensitivity C-reactive protein (hsCRP), and coronary artery calcium scoring (CACS) measured.
Participants were assigned a Framingham Risk Score (FRS), an algorithm that estimates 10-year cardiovascular risk based on age, sex, cholesterol, blood pressure, diabetes, dyslipidemia, hypertension treatment, and smoking.
Throughout the 10-year observation window, participants returned for follow-up visits twice per year where they reported their office visits, CVD medication usage, CVD diagnostic usage, and whether they were subject to any invasive procedures.

Results
While age is the most obvious cardiovascular disease risk factor, Shaw’s study found that correlations between future CVD costs and age decreased after the age of 65. Age and future CVD costs correlated closely for male participants ages 45 to 64. But male participants in the study older than 65 actually demonstrated future CVD costs that declined with age. Age and future CVD costs also stopped correlating for women participants older than 65.
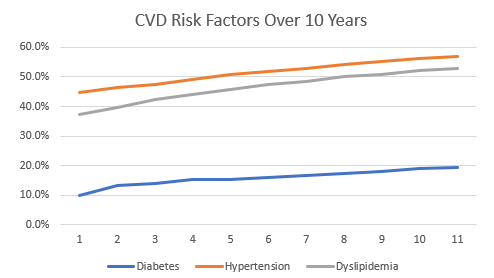
Like age, diabetes, dyslipidemia, and hypertension are also widely accepted as cardiovascular disease factors. Shaw measured the incidence of these factors throughout her study’s 10-year period, and the incidence of all three increased:
- Diabetes increased 93% (from 10% of the participants to 19.3%)
- Dyslipidemia increased 41.6% (from 37.3% of the participants to 52.8%)
- Hypertension increased 27% (from 44.9% of the participants to 57%)
Though all three factors saw substantial increases in incidence, they varied in their impact on CVD costs when compared to the study’s average 10-year CVD cost of $23,142:
- Diabetic participants incurred an average of $29,290
- Dyslipidemic participants incurred an average of $25,406
- Hypertensive patients incurred an average of $25,843
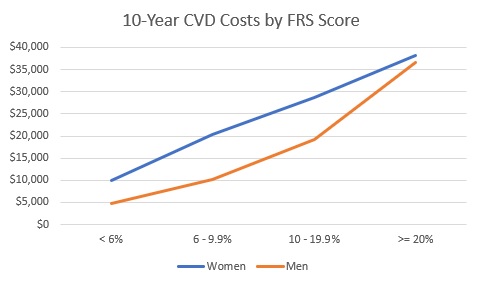
For both men and women, initial Framingham Risk Scores correlated strongly with 10-Year CVD costs observed over the life of the study. FRS improves on age as a signal by including sex, cholesterol, blood pressure, diabetes, dyslipidemia, hypertension treatment, and whether the participant has a history of smoking.
Shaw goes one step further from the strong signal FRS provided by creating low-risk, high-risk, and very high-risk buckets of study participants:
- Low-risk: FRS < 10%, CACS = 0, and normal glucose values (1,182 participants)
- High-risk: FRS ≥ 20% and CACS > 400 or diabetes (2,250 participants)
Very high-risk: FRS ≥ 20%, CACS > 400, and diabetes (126 participants)
Lower Risk Means Lower Costs
Low-risk participants of Dr. Shaw’s study accounted for 10-year average CVD costs of just $7,008, compared to $23,142 on average across the study. Despite making up 19.1% of the study participants overall, the low-risk group only contributed 5.2% of all costs.
The high-risk group, which accounted for 40.8% of the study’s participants, contributed 48% of total CVD costs. On average, they accounted for 10-year CVD costs of $37,732 in the case of high-risk women and $35,814 in the case of high-risk men. Very high-risk participants incurred 10-year CVD costs of approximately $50,000 in the case of women and $60,000 in the case of men.
The implications of Shaw’s study are extremely clear: there are substantial cost savings for both payers and providers when patients are able to avoid or delay the onset of major CVD risk factors like diabetes, unhealthy levels of fat in the blood, and high blood pressure.

Director of Finance & Operations,
Heartbeat Health